

In this post I am going to explain how the melanocortin system works. Located in the hypothalamus, this system monitors the nutritional status of our body and from there, instructs our body and brain what to do next.
Understanding the melanocortin system will help you to understand the significance of the immune complex discovered by Sergei Fetissov and his team. It will also help you to understand how this immune complex might lead to many of the symptoms of anorexia. I will also explain what he thinks this means for people with bulimia.
Inside the hypothalamus: The arcuate nucleus
There are two main structures inside the hypothalamus that regulate appetite: the lateral hypothalamus and the arcuate nucleus. In this post we are going to concentrate on the arcuate nucleus. This is the main area that monitors the body’s nutritional levels.
It’s really hard to find a royalty free image of the entire melanocortin system, because most studies focus on the satiety signalling part of the pathway, but the image below might help you to visualise what happens.
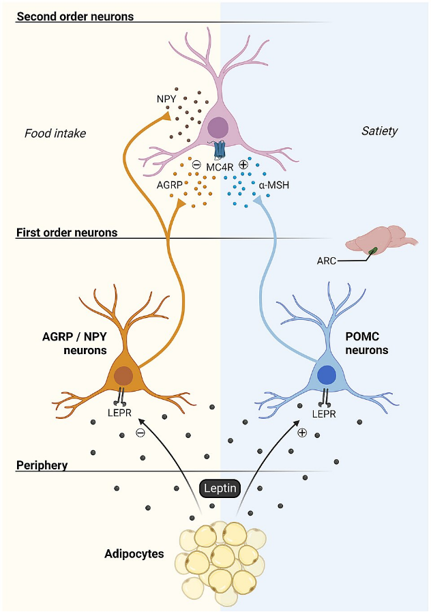
Courtesy of Olivier Lavoie, Natalie Jane Michael, Alexandre Caron, CC BY-SA 4.0.
The arcuate nucleus contains the blue and brown neurons in the image above. The blue neurons are called POMC (proopiomelanocortin) neurons. They are activated by an appetite peptide called leptin. Leptin is produced by our fat cells. The more fat in our fat cells, the more leptin we produce, broadly speaking.
The brown neurons are called AgRP/NPY (agouti-related peptide/neuropeptide Y) neurons. They are activated by ghrelin, another appetite peptide, this time made mostly in our stomachs. Ghrelin is made when we are in a negative energy balance. It could be said that leptin and ghrelin are opposite, the yin and yang of energy sensing in the body. Better nourished = more leptin, undernourished = more ghrelin.
POMC neurons produce something called proopiomelanocortin (POMC). This is chopped down into little pieces. One of these little pieces is called α(alpha)-melanocyte-stimulating hormone, or α-MSH for short.
The AgRP/NPY neurons on the other hand produce – you guessed it: AgRP and NPY.
Both the POMC neurons and the AgRP/NPY neurons project to a receptor called the MC4R (melanocortin 4 receptor), which is located in the paraventricular nucleus, or paraventricular hypothalamus (PVN or PVH). They are different names for the same thing.
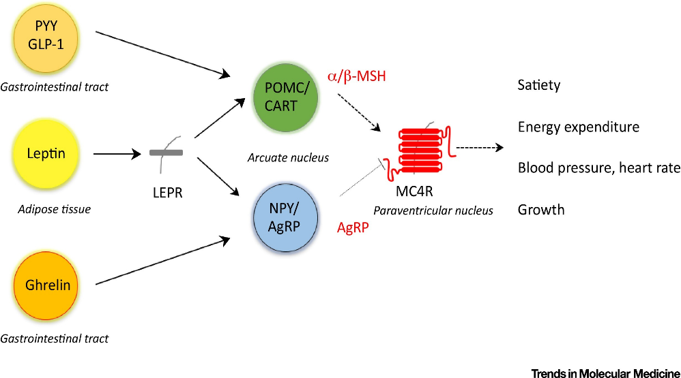
Below is another image that shows the same process. Like so many images, it is taken from a paper describing the process in obesity. But you can still see how adipose (fat) tissue = leptin = α-MSH = a satiety signal at the MC4R in the paraventricular nucleus (PVN). On the other hand, ghrelin = AgRP = an energy deficit signal at the MC4R in the PVN.
Downstream effects of melanocortin 4 receptor (MC4R) activation
As you can see from the image in the previous section, stimulation of the MC4R in the PVN, indicating positive energy balance, has a number of downstream effects in the brain and body.
One such effect will be to reduce appetite and create a sensation of satiety. Another effect is a drive to burn off all that excess energy.
In this post (link), I explained how a researcher called Sergei Fetissov at the University of Rouen in France has shown that certain strains of the Enterobacteriaceae family of gut bacteria, and specifically strains of E. coli, produce a protein that has a similar structure to α-MSH. Some people then produce an immunoglobulin to neutralise that protein. He believes in some people with these bacteria living in their guts, or who are infected with them, that their immune system mistakes this protein for their own α-MSH, binding to α-MSH, forming an immune complex. Researchers believe that this complex, α-MSH attached to an immunoglobulin, has greater affinity at the MC4R. This means that it is stickier in a way, that it binds more strongly to the receptor and cannot easily be displaced by AgRP. So even if the body is in a negative energy balance, as is the case in anorexia, and the body is producing lots of ghrelin and the brain therefore lots of AgRP, as is also the case in anorexia, the message is not getting to the MC4R.
I liken the effect this must have on how Geraldine must have been feeling in the Vicar of Dibley Christmas special, after she had eaten her third Christmas dinner in a row. In anorexia, although the body is in an energy deficit, the brain does not see it that way and thinks you, or your loved one, has eaten three Christmas dinners. And now we are asking you to eat all over again. Trials of MC4R agonists (medications that act on the MC4 receptor) cause nausea, and occasionally vomiting, as a side effect – many people with anorexia describe nausea. I can’t begin to imagine what that must feel like.
What happens in bulimia?
Fetissov has shown increased levels of this immune complex in people with anorexia, bulimia and binge eating disorder. He believes that depending on which end of α-MSH the immunoglobulin attaches (called epitope shifting), it either has greater affinity at the MC4R in anorexia, or lower affinity at the MC4R in bulimia. Can you see the N and the C at different ends of the triangle in the image below? This means that in anorexia, the immune complex binds very strongly to the MC4R and cannot easily be displaced by AgRP in anorexia. In the case of bulimia, it binds less well, and so does not send a signal of satiety to the rest of the brain and body.
The image below shows this process.
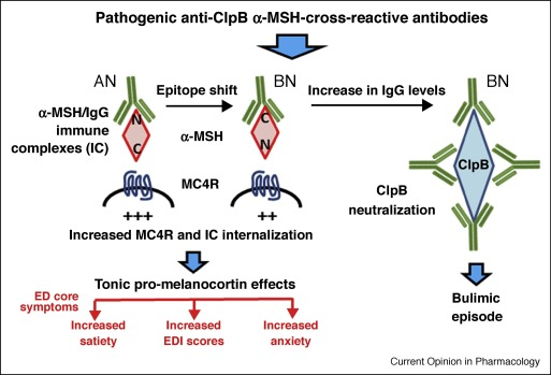
In the paper this image is taken from, the authors propose that this change in binding explains how people often switch from a restrictive eating disorder, to a restrict-binge-purge type of presentation.
What next?
The α-MSH-immunoglobulin complex is found in people both with and without anorexia, although the dynamics and the affinity of the immune complex are both different in newly diagnosed adolescents with anorexia compared with controls. While researchers initially thought that the presence of the antibodies themselves played a role in anorexia, more recent thinking (scroll down to section 3.9.2) is that the immune complex increases melanocortin signalling in people with anorexia, or perhaps the immune system fails to manage the effect of the immune complex in the way that it does in people without anorexia. This is clearly an area of active research, and we do not yet fully understand what role this immune complex plays in the development of anorexia, and possibly other eating disorders.
In many autoimmune diseases, several autoantibodies can cause the disease, or the accumulation of different autoantibodies makes it more likely that the disease will emerge. Type 1 diabetes, another autoimmune disease (which shares genetic links with anorexia), is a prime example. Several autoantibodies can lead to Type 1 diabetes, and the addition of each autoantibody increases the likelihood that Type 1 diabetes will develop, along with some environmental factors. As matters stand, my guess is that anorexia will turn out to look something like how Type 1 diabetes develops.
Want to hear more about the science of eating disorders? Sign up to receive the latest updates straight to your inbox. You’ll also be the first to know how my latest research findings might inform this area of research when these are published. I’m almost bursting with excitement and wish I could tell you now, but first to publish and all that.
For now, take care of yourself.
Elizabeth
This blog post is for informational and educational purses only and does not constitute medical nor nutritional advice. You should follow current evidence-based treatments if you or your child is suffering with an eating disorder.
Thank you to friends and colleagues, for their review of a first draft of this post.

