Recent research findings certainly seem to be pointing that way. And autoimmune disease explains many of the characteristics of anorexia: the female predominance, the relapsing-remitting or chronic nature of the illness, the surge post-Covid and even the increased risk in autism.
In this blog post I will tell you what we know so far that points to autoimmunity as the cause of anorexia.
I will start by showing you two of the larger studies showing an association between eating disorders and other autoimmune diseases (there are several smaller ones). We will then look at another large population study that showed a link between eating disorders and both infections and the use of anti-infective agents (like antivirals and antibiotics) in teen girls. We’ll skip on to explore some funky research produced by two separate research teams in Europe – each one has discovered different autoantibodies in anorexia. I will show you how these autoantibodies might explain some of the cardinal symptoms of the disease.
The post finishes with the question “What now?” What does this mean for someone struggling with anorexia, or watching a loved one suffer. And what needs to happen next before we have truly effective treatments for the disease?
Population studies show an association between eating disorders and autoimmunity
There are several population studies that show a link between eating disorders and autoimmune disease. I will mention two of the most important ones here.
The first study, reported in 2017, included all children born in Denmark to Danish-born parents between 1989 and 2006 who were alive and residing in Denmark on their sixth birthday. A total of 930,977 children were included, of which 48.7% were girls.
The authors looked at hospital data reporting on in-patient and out-patient episodes and compared any report of an eating disorder (anorexia nervosa, bulimia nervosa and eating disorder not otherwise specified (EDNOS)) against recorded instances of 50 different autoimmune and 10 autoinflammatory diseases. These diseases included the most common autoimmune diseases, such as rheumatoid arthritis, systemic lupus erythematous (SLE), Crohn’s disease, coeliac disease and Type 1 diabetes, to the rarer diseases, like Churg–Strauss syndrome and Schnitzler/Muckle–Wells syndrome. They also looked at whether teens were more likely to have an eating disorder if their parents had a history of autoimmune or autoinflammatory disease. I’ve listed all of the diseases included in a table at the end of this blog post. My guess is you are going to look at the list and be able to pick any number of these that run in your family. I see this in the patients that I meet.
The authors of the study discovered that there was a 36% higher hazard for anorexia nervosa if a child or adolescent had one of the autoimmune or autoinflammatory conditions examined. Put another way, this means that a child or teenager was 36% more likely to have anorexia if they also had any one of these autoimmune or autoinflammatory conditions. The hazard ratio was even higher for bulimia and EDNOS: 73% for bulimia nervosa and 72% for EDNOS.
Parental autoimmune or autoinflammatory disease history was associated with significantly increased odds for anorexia nervosa, 1.13 (so 13% more likely to develop anorexia if a parent had a history of autoimmune or autoinflammatory disease). Again, the odds of bulimia and EDNOS were stronger still: 1.29 for bulimia and 1.27 for EDNOS.
The second study used the Swedish population and included more than 2.5 million individuals born in Sweden between January 1, 1979, and December 31, 2005, and followed up until December 2013. This study showed that, in males, any preceding autoimmune disease was associated with an 82% increased hazard in Other Eating Disorder (OED) and a 78% increased hazard in Any Eating Disorder (AED). In females, any preceding autoimmune disease increased the hazard for anorexia by 59%, for OED by 71%, for AED by 62%, and for bulimia by 57%. In turn, anorexia, bulimia, and OED increased subsequent hazards of autoimmune diseases.
One could take these findings and assert that maybe the malnutrition of an eating disorder increases the risk of autoimmunity. Maybe. But I don’t think that’s very likely. Generally speaking, having one autoimmune disease increases the risk of having another.
A link between infection and eating disorders
In this section, I’m going to talk you through a third large study that examined the link between infections, anti-infective agent use (like antibiotics and antivirals) and eating disorders in adolescent girls.
The study population consisted of 525,643 girls born in Denmark from January 1, 1989, to December 31, 2006, and followed up until a mean age of 16.2 years. Infections included sepsis, liver infections, infections of the gastrointestinal tract, the skin, lungs, ears and central nervous system, and also urological and genital infections.
The charts below show the association between any infection and each of the eating disorders, and anti-infective use and eating disorders. As you can see, the risk of anorexia after a hospitalisation with an infection increases in the immediate 0–3-month period after hospital contact and then attenuates (gets less likely to cause anorexia) with the passage of time and has almost disappeared after 5 years. As an aside, I will fairly soon be able to share our own research findings regarding a very specific infection, so sign up to get alerts.
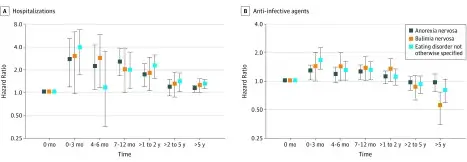
Regarding the anti-infective agents, I often get asked “Is it the medications themselves?” Maybe. But anti-infective agents like antibiotics and antivirals are also an indicator of an infection, so perhaps it is infection itself. You don’t generally get prescribed one unless you have an infection, especially in a country like Sweden. The authors did control for this in their analysis however.
The researchers followed up with analyses of gastrointestinal infections specifically, which showed that the risk of a diagnosis of EDNOS may be greatest after a hospital stay for a gastrointestinal infection: history of a hospital stay for a gastrointestinal infection was associated with a 60% increase in EDNOS (hazard ratio 1.60). Sign up if you want to hear more about my thoughts on this research in ARFID and the dangers of psychologising this condition in the same way as we have for anorexia.
Specific autoantibodies in anorexia (and other eating disorders)
Two important questions remain from these research findings:
- Which infections might trigger eating disorders? Any infection, or specific infection(s)?
- What part of the brain, what cell type, what receptor is involved in a possible autoimmune response?
I have a hypothesis regarding the first question, and it is an area of active research, findings to be published soon. Turns out my hunch may be right. Sign up to be notified when this happens.
As to question 2, let’s look at the specific antibodies two different research teams in Europe have discovered.
The first, and the area with the most research, is the immune complex discovered by Sergei Fetissov and his team at the University of Rouen in France. He has discovered that the Enterobacteriaceae family of gut bacteria, including certain strains of E. coli, produce a protein, caseinolytic protease B (ClpB), that looks quite similar to our own α-MSH. (Read here on the melanocortin appetite regulatory system in the hypothalamus.) He believes that in some people with these bacteria living in their guts, or who are infected with them, their immune system mistakes this protein for their own α-MSH, binding to α-MSH, forming an immune complex. Increased levels of this immune complex have been found in people with anorexia, bulimia and binge eating disorder. Plasma levels have been correlated with the severity of psychopathological traits as measured by the EDI-2 scale. Interestingly, plasma concentrations of ClpB correlate positively with perfectionism in non-clinical samples, i.e. people without an eating disorder.
In anorexia, this immune complex has greater affinity at its receptor, the MC4 receptor.
In plain English, this means that it binds to the receptor more tightly, it is stickier so to speak. In contrast, it is less sticky in people with bulimia and binge eating disorder. If you have read the post where I explain the melanocortin appetite regulatory system, you may now understand the significance of this finding.
An immune complex that is bound to the MC4 receptor that is stickier than our own α-MSH sends a message to the rest of the brain, and the body, telling the brain that the body is in positive energy balance even when it isn’t. Can you envisage what the net effect of this might be? A false message that you do not need to eat. Your brain perceives that you have just eaten the equivalent of a Christmas dinner and the thought of eating anything else is impossible. Probably an urge to burn off all that excess energy too, as we know that when this receptor is stimulated in rodent models, they are compelled to wheel run. Enhanced melanocortin tone also drives anxiety (reviewed here).
The image below describes this theory and these findings for those of you who are more visual.

This research is particularly intriguing if you consider the third study discussed earlier in this post: the association between infections, of which some will be gastrointestinal, anti-infective agents and eating disorders in teens.
The caveat with Fetissov’s research is that this immune complex is found in people without anorexia also (scroll down to section 3.9.2 of this paper for an up-to-date review) and is correlated with BMI (higher levels of the immune complex = lower BMI). This does not mean it is not relevant. For some autoimmune diseases, people may have antibodies but not develop the disease itself. Positive ANA antibodies for lupus (SLE) are one such example. In others, such as Type 1 diabetes and coeliac disease, there might be environmental triggers, often infections, that take someone from genetic predisposition, to antibodies, to disease. Sometimes having one infection or antibody increases the chances of getting another one, leading eventually to the disease. Type 1 diabetes is again an example of this. Does some other infection dysregulate the immune system in anorexia, so that for those with E. coli strains in their intestines, something that is normally protective or functional, by suppressing appetite and excess weight gain so as to remain at a healthy weight, becomes dysfunctional?
This leads us to consider the findings of the second research group. Daniele Saverino’s team at the University of Genoa in Italy have discovered an antibody that targets an as yet unknown part of the hypothalamus in people with anorexia. In 2024 he expanded his sample to 48 people with anorexia and compared them to 48 controls without anorexia and found that every person with anorexia had the antibody.
Six people without anorexia also had the antibody, but, as discussed above, in some autoimmune diseases a small number of people may have the antibody without developing the disease – there is often another trigger needed for full-blown autoimmune disease. This can be environmental factors and/or another infection, the so-called “two-hit” hypothesis. Perhaps both Fetissov’s immune complex and Saverino’s anti-hypothalamic autoantibody are needed for anorexia to develop.
These research findings are a big deal for anorexia, and other eating disorders, and I am surprised so few people are aware of them. Saverino’s research may mark the beginning of an eventual diagnostic test, much like ANA is used, alongside clinical findings, to diagnose SLE. It might also mean that one day there will be a medication that blocks, binds or neutralises this antibody.
What next?
What does this mean for a person, or for you if you are caring for a loved one, with anorexia? While this information might not offer immediate solutions, it may help to understand this is not a disease of your mind. You are not flawed, your mind is not fragile, you are neither hysterical nor weak. Rather your immune system has responded in an unhelpful way, probably to an infection or infections, that arrived just at the wrong time, and attacked an as yet unknown part of a cell in your brain, probably somewhere in the hypothalamus. The infection, or the immune system’s attack, has quite probably affected parts of the brain involved in size and shape perception (more on this to come in future posts – you know what to do).
What part of a cell does Saverino’s autoantibody target? In time we will understand the exact part of which cell is involved. This will mean the commercialisation of a diagnostic test, which will come with the message to everyone: “This is real. It is a biological process. I am not mad/weak/ “mental”. A bit like tissue transglutaminase (tTG) for coeliac disease screening maybe.
From there, researchers will be able to create medicines, treatments that actually work. Like the biological treatments available today for Crohn’s, for ulcerative colitis, for rheumatoid arthritis. While not always perfect, they at least offer relief where a decade ago there was little.
Perhaps, hopefully, researchers will be able to repurpose existing treatments. One such class are the biological medications for other autoimmune diseases. A handful of case reports have shown resolution of anorexia in patients who have been prescribed medications to treat a co-existing autoimmune disease. These medications come with a warning though, which I will explain in another post.
For now, what this emerging research tells us is that anorexia is a biological disease. It has a biological explanation. It’s NOT all in your head.
Until next time, take care of yourself.
Elizabeth
This blog post is for informational and educational purposes only and does not constitute medical nor nutritional advice. You should follow current evidence-based treatments if you or your child is suffering with an eating disorder.
Thank you to friends and colleagues, for their review of a first draft of this post.